The Great Cholesterol Scam and The Dangers of Statins
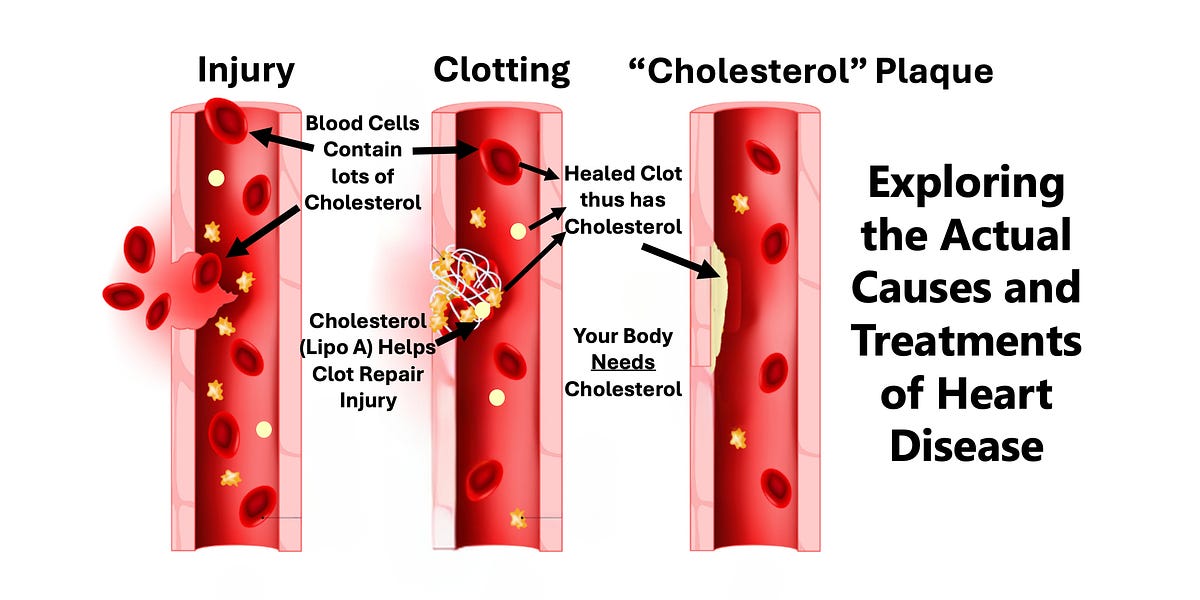
Exploring the Actual Causes and Treatments of Heart Disease

Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
Post any issues in the thread below or reach out directly to support!
View thread Contact support
I have the same issues low HDL, the LDL isn't high either, my Tri-glycerides are high and have always been high for at least the last 30 years. I have pain issues with all statins, the latest being Livalo, which raises blood sugar and some muscle pain from time to time. I am 69, I have had a blockage 14 years ago with stents placed in one artery, cardiologist always asks if I exercise and I always reply "not intentionally". I am on regular bp meds and omega 3's, coQ10 etc. I am at the age where I feel like what's the use to jump through the hoops, take the meds, empty my bank accounts and just quit all meds and wait for the big one to hit. I think I should lower my doseage of fuckitall before I get too depressed.I'm not a doc, but I have some knowledge of meds, including statins. I have a bottle of generic Atorvastatin sitting on my shelf collecting dust, that was prescribed initially by my PCP. Although, to be fair, she did say it was "optional" if my standard cholesterol level didn't drop (which, thankfully, it has).
My general cholesterol level has been pretty good, over time. What I need to work on now is lowering my Tri-glycerides (just beyond the "reference range," right now), and raising my HDL (it's OK, but could be higher). I did get a CAC scan last year which fell into the "mild" range now, but we'll see again later this year.
I have the same issues low HDL, the LDL isn't high either, my Tri-glycerides are high and have always been high for at least the last 30 years. I have pain issues with all statins, the latest being Livalo, which raises blood sugar and some muscle pain from time to time. I am 69, I have had a blockage 14 years ago with stents placed in one artery, cardiologist always asks if I exercise and I always reply "not intentionally". I am on regular bp meds and omega 3's, coQ10 etc. I am at the age where I feel like what's the use to jump through the hoops, take the meds, empty my bank accounts and just quit all meds and wait for the big one to hit. I think I should lower my doseage of fuckitall before I get too depressed.
My BP meds have been adjusted. I take Losartan and Amlodipine.
I have watched on TV some motorcycle races. A guy lays down his Kaw 750 at 120 MPH and scoots himself away and takes a couple of rolls, a few layers off the leathers. And he was wearing a helmet.It is not debunked at all, but you could make an argument that it is overstated.
It is overstated because your doctor in general will tend to act as though take this medicine and you will live, and don’t take it, and you will die. As I noted above, the absolute reduction in the probability of an event that these drugs prevent is quite small.
It is very similar honestly to motorcycle helmets. Every doctor and public health person is going to tell you man you gotta wear your helmet or you’re gonna get all fucked up. And you’re one of these dudes that’s been rolling around on his Harley without a helmet for 30 years. You’re gonna tell him he’s full of shit.
Statistically, you should wear your helmet because if you have an accident, you’re probably gonna get all fucked up If you don’t wear one. On the other hand, the probability of a severe accident is thankfully quite low so you can roll the dice and get away with it for a long time maybe your whole life.
So even though on the population level, wearing a motorcycle helmet might prevent Thousands of brain injuries and deaths every year, on the individual level the risk of a crash is relatively small and the benefit of a helmet is smaller still
Later, I will go link a post on my blog about this exact issue. That is titled “what is good for the population might not be good for the patient”
That is the crux right there: doctors are trying to benefit the population as a whole, where that these tiny little benefits for each patient get magnified by all of the patients they are treating. Often on the individual level, the benefit is quite small.
I pee a lot, as well, though that was a symptom before all this. I have also learned to take probiotics and to drink one Gatorade a day. I still drink coffee and tea. But I want to keep up minerals, etc.I'm not so far away from you, age wise (will be 67 in Nov.). This whole cardio thing started for me a year ago during my Medicare "Annual Wellness Exam." My PCP finally decided to do a 12-lead and it came back with a RBBB (Right Bundle Branch Block). So, I got the Cardiologist referral. They did a whole bunch of tests (including the CAC scan, which I anted anyway), and also including a chemical version of the cardiolyte stress test, where they shoot you with this radioactive stuff that makes you go funky for a minute or two. That came back totally normal. And the CAC was in the "mild" range. In summary, the Cardiologist indicated that the RBBB was normal in about 30% of patients and nothing to worry about. He did put me on low dose Aspirin, once per day. He indicated that the best way to reverse the CAC results would be a "plant based diet." (Yeah, Right!).
So, do I. Plus Hydrochlorothiazide (diuretic). It does make you Pee a lot. Well, a lot more than "normal." I should say. That, and I'm also on "Farxiga" for Type II, plus the standard Metformin and Glipizide. I have noticed a bit of weight loss with the Farxiga, which is good. I just with they'd release a generic version as it costs about $450.00 for a 90 day supply.
I pee a lot, as well, though that was a symptom before all this. I have also learned to take probiotics and to drink one Gatorade a day. I still drink coffee and tea. But I want to keep up minerals, etc.
 dark roast whole bean which I grind) in the morning, both with raw Sucralose (NOT with Splenda - it's cut with Maltodextrin which makes it a sugar). Then it's just a matter of keeping as much sugar as I can out of my diet. It won't be a complete removal, but I try to get as close as I can.
dark roast whole bean which I grind) in the morning, both with raw Sucralose (NOT with Splenda - it's cut with Maltodextrin which makes it a sugar). Then it's just a matter of keeping as much sugar as I can out of my diet. It won't be a complete removal, but I try to get as close as I can.I’m not from the Midwest and I don’t claim to be a genius, nor did I tout my bonafides of being trained at a venue “considered to be the best in the world” at anything. i also missed your name and medical license number in your post. I first thought you were referring to me and not the guy who wrote the article, but it’s about the same either way.There’s always gonna be some dude like this Midwest Doctor who doesn’t offer his name who presents himself as the genius who cracked the great conspiracy in medicine. I have been very skeptical of just about everything I have ever learned in medicine, but most of it honestly represents the best state of knowledge at a given time, with some notable exceptions. Cholesterol is not an exception.
I went to my doctor. He said I have high cholesterol. I said that I wanted a second opinion.I assume you’re talking about me. I’m not from the Midwest and I don’t recall claiming to be a genius anywhere, nor did I tout my bonafides of being trained at a venue “considered to be the best in the world” at anything. I believe that part was you friend. I also must have missed your name and medical license state and number in your post.
I didn’t encourage anyone to do anything other than educate themselves about the benefits of real whole grains. On the contrary, I believe I clearly relayed I’ve been somewhat humbled since my medical education (class of 2004).
To be perfectly clear, I am saying I don’t really know anything for sure, except the fact that I know I don’t know it all. A lot of the premises I previously built my world view on have been shattered by my own practical experience.
To rebut your suggestion that I am a conspiracy theorist, let me give a very specific example. Once upon a time, I very regularly used a product called hetastarch. It went under the brand name Voluven. It was a synthetic colloid that could be used for volume resuscitation in surgical or critically ill patients. I really liked it because it was cheap (an alternative to human albumin, very $$$), and I could give it quickly, unlike albumin which came in non pressurizable glass bottle containers at the time. FDA approved, on formulary at my institution, safe and effective.
One day, I went to get some hetastarch and lo and behold, it was pulled from the pharmacy and I learned it had been taken off the market. Why, you might ask? Because a guy named Joachim Boldt, a physician considered to be a leading expert on medicinal colloids (probably trained somewhere considered to be “the best in the world”, lol), had outright lied and falsified his data when the product was being trialed. Meta analysis of trials excluding his data showed an increase in mortality and acute kidney injury when using hetastarch. It was literally killing people, this guy KNEW IT AND DIDNT CARE!!!!! I know he was an anesthesiologist, but do you suppose he’s the only crook in all of medicine? That’s pretty gullible for a guy trained at the best place in the world for anything. How much money do you think was spent on Voluven vs how much gets spent on Crestor world wide?
There are other examples, like the decade we spent telling everybody they had to be on beta blockers because it decreased your risk of a heart attack. It was awesome until we figured out that was true, except they instead increased your overall risk of death, but from a stroke, not an MI. Trust the science. Lol somebody get me an epidemiologist.
Let me use your statement about why not just take it and get on with life from a different perspective. If you’re big pharma, and you can make a drug, and maybe it helps some people, maybe it hurts some people, but you can make billions of dollars by convincing everyone they need it, why not just MAKE it and get on with life? See how that works?
Men lie, institutions and governments mislead for money, power, and control. The Tuskegee experiments, MK ultra, operation sea spray, operation whitecoat, HIV/AZT studies in Zimbabwe, phizer’s Trovan trial in Nigeria, operation mockingbird, operation paper clip, Nayirah Al-Sabah, the gulf of Tonkin, on and on and on. I wish there was an avatar truth and virtue out there, but I believe the only one we had was crucified by the government some time ago.
Let me close by being extra crystal clear. I am not trying to dissuade anyone from veering from the advice of their healthcare professional. I’m just speaking my heart. I wish I didn’t feel this way. Any man is free to do as he sees best. Take your statin, take your SSRI, get your booster. If fact, forget everything I said.

That's why we randomize, and do post-hoc statistical tests of differences in, eg, flatulence rates between active treatment and placebo, to determine if the differences observed are greater than what would be expected by chance alone.The problem I have had with studies is also their strength. a group of people are tested. One gets the real thing, one gets a placebo.
The idea is to see what the medicine actually acomplishes.
But you will see that the medicine comes with warnings like may cause incessant flatulence or dryness of mouth. Things that may have been reported by patients and had nothing to do with the meds on trial. Just a guy who is gassy and thirsty all the time but they cannot report it like that.

Vitamin K2 activates a protein called matrix GLA which removes calcium from soft tissues and it also activates osteocalcin, which holds calcium to bone. So, if you have a lot of calcium, you need vitamin K2 to direct it. Think of parking attendants at large events; they tell you where to put your car. K2 tells you where to put calcium. When it comes to calcium, where it ends up is what counts, not how much you have.I don't even know what vitamin K2 is. But here's the USPSTF current recommendations on Vit D and Calcium (spoiler: not recommended)
Your credentials, please.Statins are evil. Do you know what else was a big scam? Telling young thin women of European descent that they needed to take calcium in large doses without Vitamin K2 to prevent osteoporosis. Calcium builds up straight in the large arteries without the K2.
I'll be 58 tomorrow.I’m amazed at the turn I’ve taken in the last 10 years. Back then, I thought you couldn’t survive past 60 without a statin, and ACE inhibitor, and probably an SSRI.
I'll be 58 tomorrow.
I've never been on any medications in my life.
I'm in better physical condition than when I left the Navy 30 years ago.
I'll be fine in two years time. And in ten.
Dude they’re $4 a month and millions of people are on them but your mind is obviously made up so carry onBoth the folks I know who were put on statins... quit almost immediately. Said it fucked them up.
Avoid at all costs. Once they get you on them... it's a cash cow.
My plan is for stents, bypass, transplant... whatever. But no fucking Statins. For the last 20 years I've looked at that shit and said "No FUCKING Way!"
Sirhr
Since you were at HUP you ought to know that you cannot take all that basic science mumbo jumbo and make strong clinical inferences from it.Vitamin K2 activates a protein called matrix GLA which removes calcium from soft tissues and it also activates osteocalcin, which holds calcium to bone. So, if you have a lot of calcium, you need vitamin K2 to direct it. Think of parking attendants at large events; they tell you where to put your car. K2 tells you where to put calcium. When it comes to calcium, where it ends up is what counts, not how much you have.
Skeletal formation and prevention of soft tissue calcification
Vitamin K-dependent γ-carboxylation is essential to several bone-related proteins, including osteocalcin, anticoagulation factor protein S, matrix γ-carboxylated glutamate (Gla) protein (MGP), Gla-rich protein (GRP), and periostin (originally called osteoblast-specific factor-2). Osteocalcin (also known as bone Gla protein) is synthesized by osteoblasts (bone-forming cells); the synthesis of osteocalcin is regulated by the active form of vitamin D, 1,25-dihydroxyvitamin D (calcitriol). The calcium-binding capacity of osteocalcin requires vitamin K-dependent γ-carboxylation of three glutamic acid residues. Although its function in bone mineralization is not fully understood, osteocalcin is required for the growth and maturation of calcium hydroxyapatite crystals (see Osteoporosis) (11).
Protein S appears to play a role in the breakdown of bone mediated by osteoclasts. Individuals with inherited protein S deficiency suffer complications related to increased blood clotting, as well as osteonecrosis (12, 13). Protein S can bind and activate receptors of the TAM family that are involved in phagocytosis. Mutations in TAM receptors can result in visual impairment, defective spermatogenesis, autoimmune disorders, and platelet disorders (14).
MGP has been found in cartilage, bone, and soft tissue, including blood vessel walls, where it is synthesized and secreted by vascular smooth muscle cells. MGP is involved in the inhibition of calcification at various sites, including cartilage, vessel wall, skin elastic fibers, and the trabecular meshwork in the eye (see Vascular calcification) (15, 16). Moreover, several VKDPs, including MGP, have been associated with calcification sites in arteries, skin, kidneys, and eyes in certain inherited conditions, such as pseudoxanthoma elasticum and beta-thalassemia (17, 18).
The vitamin K-dependent proteins, GRP and periostin, are also synthesized in bone tissue, but their roles in bone metabolism are still unclear (19, 20). Expressed in normal human skin and vascular tissues, GRP has been colocalized with abnormal mineral deposits in the extracellular matrix in calcified arteries and calcified skin lesions (21). Expressed in most connective tissues, including skin and bone, periostin was initially associated with cell adhesion and migration. This VKDP also appears to promote angiogenesis (formation of new blood vessels) during cardiac valve degeneration and tumor growth (22, 23).
Current research suggests that reduced γ-glutamylcarboxylase activity and/or lower vitamin K bioavailability may impair the activity of VKDPs and contribute to bone mineralization defects and abnormal soft tissue calcification (see Disease Prevention) (24).
I don’t even know where to begin. OK, I will begin with my credentials. I graduated medical school 26 years ago and 22 years ago I got a masters in public health with a concentration in epidemiology from Johns Hopkins Bloomberg School of Public health, considered the best in the world and I have done plenty of meta-research which means researching research and its methodology. I have actually written a lot on my blog....
I don't even know what vitamin K2 is....


I'm not so far away from you, age wise (will be 67 in Nov.). This whole cardio thing started for me a year ago during my Medicare "Annual Wellness Exam." My PCP finally decided to do a 12-lead and it came back with a RBBB (Right Bundle Branch Block). So, I got the Cardiologist referral. They did a whole bunch of tests (including the CAC scan, which I anted anyway), and also including a chemical version of the cardiolyte stress test, where they shoot you with this radioactive stuff that makes you go funky for a minute or two. That came back totally normal. And the CAC was in the "mild" range. In summary, the Cardiologist indicated that the RBBB was normal in about 30% of patients and nothing to worry about. He did put me on low dose Aspirin, once per day. He indicated that the best way to reverse the CAC results would be a "plant based diet." (Yeah, Right!).
The point is the thread is being derailed severely by references to irrelevant nonsense, such as iso forms of vitamin K that have unknown relevance to human health.
I suggest we stay on topic if anyone wants to get anything of value out of this thread
I was talking about the Midwest doctor in the original blog post in the original post in this thread
Hetastarch is a pretty niche example kind of like Xigris. I don’t think that is a good comparison for something like statins, which have been studied extensively for going on 40 years. In fact, it is one of the best studied things in medicine with consistent results nearly across-the-board with the exception of Vuitton. But of course that’s not a statin
And John Hopkins is the number one school of Public health in the country. I am simply stating credentials and facts because too often a lot of this contrarian stuff you find on topics like this is promoted by quacks with questionable credentials or expertise.
Dr Nadir Ali is a cardiologist and is as transparent as they come about his opposition to statins for absolutely everyoneI don’t even know where to begin. OK, I will begin with my credentials. I graduated medical school 26 years ago and 22 years ago I got a masters in public health with a concentration in epidemiology from Johns Hopkins Bloomberg School of Public health, considered the best in the world and I have done plenty of meta-research which means researching research and its methodology. I have actually written a lot on my blog about the cholesterol hypothesis some of it skeptical. My skepticism evaporated when the PCSK9 inhibitor studies came out.
Bottom line is this: if it is for what is called primary prevention, meaning that you don’t have heart disease already, but you have certain risk factors which are usually judged by what is called the Framingham score. If your score is high, it means you’re predicted to have something like let’s say a 10% risk of a major cardiac event Happening in the next 10 years. They would probably recommend a statin under those circumstances. However, it is true that your risk in the next 10 years goes down from the original predicted 10% to statistically something like 9%. Meaning that your absolute reduction in risk is indeed quite small and whether or not, you take a statin you still have almost a 10% risk of the bad shit happening. In a case like that, if it were me, and the statin didn’t cost much didn’t inconvenience me much and didn’t cause me severe muscle cramps, I would just take it and get on with Life because why not?
On the other hand, if you already have heart disease, they will give you a statin for what they call “secondary prevention“ which basically means preventing more events like heart attacks in the future. Under those circumstances, you stand to benefit a lot more from taking the statin. I can’t give you a number right now, but I think that you would be a damn fool not to take it
There’s always gonna be some dude like this Midwest Doctor who doesn’t offer his name who presents himself as the genius who cracked the great conspiracy in medicine. I have been very skeptical of just about everything I have ever learned in medicine, but most of it honestly represents the best state of knowledge at a given time, with some notable exceptions. Cholesterol is not an exception.
I’ll tell you this also: now that I’m over 50, I tell the young doctors that I train in the hospital where I work when I reflect back on the good old days, I say “I grew up in the days when men were men and MIs were transmural”. A transmural myocardial infarction is a big one that goes through the whole wall of the heart not just the lining. When I started back in the late 90s, we got lots of transmural myocardial infarction. People had huge heart attacks and they got super fucked up from them. Heart failure, and basically becoming a cardiac cripple.
You don’t really see that much anymore. Our armamentarium of medication’s to prevent heart disease, and our interventions to treat heart disease like stents and blood thinners, and so on has become so powerful as that, it has changed the nature of the disease. You can shrug off a lot of that as a big conspiracy, but you do so at your own risk.
If you guys want to read some stuff by a legitimate skeptical cardiologist who’s not just trying to stir up conspiracies, and who is respected as and among mainstream cardiologists, go find the blog of a country cardiologist in Kentucky named John Mandrola MD. He’s a guy that you can trust completely (I know him.)

 www.youtube.com
www.youtube.com
Dr Nadir Ali is a cardiologist and is as transparent as they come about his opposition to statins for absolutely everyone
Eat Mostly Fats
THANK YOU SO MUCH FOR WATCHING AND SUPPORTING US! Dr Nadir Ali is currently not offering Online Consultations. Email us at [email protected] Website: www.eatmostlyfat.com Facebook group: http://bit.ly/eatmostlyfatsfb\ Thank you! EMF Team **All videos on this channel are edited and...
Am I lying, or mistaken? Please enlighten me as to my error. I must have missed something by not going to drug rep school.Dude.
Next time lead with this.
P
There is no clinical relevancy for K2. I am at a university hospital right now and no physicians even know what it is among the ones I casually queriedBut you bring up Xigris and motorcycle helmets..there is tons of clinical relevancy for K2.
Please provide a link to the circulation paper that you claim you authored; I just want to make sure it was not a letter to the editor about nattokinase or some other fringe quackery treatment. Because that’s what nattokinase is and if you are truly a physician recommending these fringe treatments, you have exposed yourself as a shill of the vitamin/supplement/alternative medicine movementThere is a role in severe (esp. familial) hypertriglyceridemia - that being said I am aware of AHA guidelines for even "moderate" elevated triglycerides.
For a long time they weren't $4, they were a cash cow that IMHO was overprescribed. I would recomend nattokinase for plaque reduction over statins. All medicine should be risk/benefit ratio. But big Pharma not profiting...
The posts are over 10 years old. Do you have any more recents posts?Here's another blog post I wrote about statins called
Billions and Billions of People on Statins? Damn the Torpedos and Full Speed Ahead
Billions and Billions of People on Statins? Damn the Torpedos and Full Speed Ahead
A blog about biases in the conduct, interpretation, and application of evidence from clinical trials in medicinewww.medicalevidenceblog.com
Please provide a link to the circulation paper that you claim you authored; I just want to make sure it was not a letter to the editor about nattokinase or some other fringe quackery treatment. Because that’s what nattokinase is and if you are truly a physician recommending these fringe treatments, you have exposed yourself as a shill of the vitamin/supplement/alternative medicine movement

Those post are about risk appraisal and behavioral choice regarding to health risks. They’re not exactly going to change overtime.The posts are over 10 years old. Do you have any more recents posts?
